Welcome to the Afibber’s Forum
Serving Afibbers worldwide since 1999
Moderated by Shannon and Carey
 |
 |
 |
 |
 |
 |
|
Keto diets and afib April 25, 2016 03:06AM |
Registered: 11 years ago Posts: 4,324 |
In this post: <[www.afibbers.org] , Lynda asked me to explain my caveat about keto diets for afibbers.
For those who aren’t familiar. Here is a description of keto diets. This is by a type 1 diabetic, who is an MD and uses a keto diet to manage his diabetes: <[ketogenicdiabeticathlete.wordpress.com]
It has to do with electrolyte shifts that occur when someone transitions into a ketogenic state. This is a low insulin state. When insulin is high, the insulin signals the kidneys to conserve or retain sodium. When insulin drops to very low (and in my opinion, normal) levels, the kidneys are signaled to excrete sodium (called natriuresis of fasting). This can be dramatic enough that the body excretes potassium along with the sodium – trying to keep them in balance (body will secrete the hormone aldosterone causing it to excrete potassium). For more detailed explanation, see the books by Phinney and Volek <[www.artandscienceoflowcarb.com] They recommend supplementing with 5g/day of sodium, at lest 1g/day of potassium and also magnesium.
Most peoples’ ketone system are in “mothballs” since many fuel on a mostly carb diet to continually fill up the small glucose tank in the body. It can take up to 2 or more weeks of starvation or a very low carb (generally 20 or 30 g/day or less) diet with modest protein to stimulate the body to bring this system out of mothballs. The body first empties the glycogen stores in the muscles to feed the brain (which can only fuel on glucose or ketones). Once these are depleted, muscle protein is converted to glucose for this purpose (muscle tissue can fuel on fat). After a while the body starts making ketones from fat and these ketones can offset much of the brain’s need for glucose.
Ketones are not produced in a high insulin state.
In my case, I did not know about the sodium supplementation recommendation. I dropped my carb intake to around 20g/day. I got all the symptoms of “keto flu” (which can be mitigated with appropriate supplementation). After a few days, I noticed a “pounding heart” when I went to bed. This is typically a symptom of low potassium, so I loaded up on it – I don’t recall, but likely 4-5 grams/day. This continued for a couple of days. One evening I thought, this will lead to afib. Sure enough I woke up with 3 AM afib. I converted it in about an hour with 300 mg of flecainide (as usual). Except this time I converted to a rate of around 130 BPM (my normal rate after a flec conversion is in the 80’s). This stayed this way for a while. I got the idea to take a bunch of magnesium (as this was 6 years ago, don’t recall how much, likely 400-800 mg). I did and within 10 minutes, my rate started dropping into the 80’s. I took a while, but I think less than 30 minutes.
That was in Oct of 2009. I’ve been keto-adapted since, though have gone in and out of ketosis many times. I’ve yet to have another afib episode related to this. I also likely get less than 5 g/sodium/day. All food is cooked from scratch. I do add salt, but not a huge quantity.
As to why I think a low insulin diet is healthy. It starts with Dr. Joseph Kraft. You can read his book - <[www.amazon.com] A summary is here: <[www.thefatemperor.com] Bottom line – Kraft did 14,000+ oral glucose tolerance tests WITH insulin assays. He found that 80% who had normal glucose responses had abnormal insulin responses. He called this “diabetes in-situ.” This does not count all those who had abnormal glucose responses. You need a fasting insulin of 5 or less to be in the clear. Kraft also did 3,000 autopsies and saw that excess insulin was the cause of much calcification in the heart, its structures and blood vessels. So keeping insulin low is a hot option. Here is an interview with him – he’s 96 and first published on this around 1976. <[www.youtube.com] Catherine Crofts, in NZ, used the Kraft data for her PhD thesis recently. Here is a presentation by her : <[www.thefatemperor.com]
In this post, they cite a study demonstrating that fasting insulin represents 50% of total insulin secretion for the day. This relationship holds for those with low and high levels. Hence someone with a fasting insulin of 30 produces 10 times the insulin over the course of a day as someone with a fasting insulin of 3. <[www.buttermakesyourpantsfalloff.com]
The guys at Newcastle showed they could normalize glucose function by reducing fat around the pancrease (it is organ fat, not subcutaneous fat that is the issue) <[www.sciencedaily.com]
In Hans’ newsletter, the editor did n=1 experiments with the Newcastle approach. Here is a search on the archives: <[www.google.com]
Toronto doc, Jason Fung, talks about insulin and obesity <[intensivedietarymanagement.com]
And has a many part section on fasting, staring here: <[intensivedietarymanagement.com]
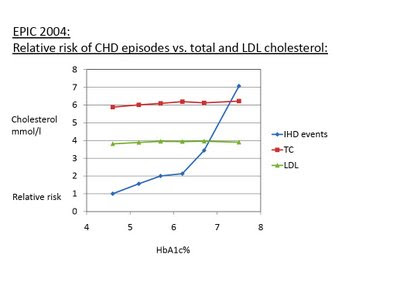
This is an old post, analyzing an older paper. <[high-fat-nutrition.blogspot.ie] However, he plotted the data to highlight the risk of coronary heart disease risk vs A1C levels
In summary – I think low insulin levels are a healthy way to live. As to afib, there is risk to going into ketosis. If you want to try it, make sure you pay attention to the electrolyte supplementation best practices. Can you get into ketosis slowly and mitigate the risk? I don’t know, I’ve not tried it. I have a friend who said she did. I’ve also read that it isn’t possible. I don’t know the answer. Will it help your afib? Perhaps, especially if you have comorbidities like hypertension and coronary artery disease. It was not a ticket out of afib for me. I already had that ticket to afib remission- primarily magnesium to bowel tolerance, but also taurine and earlier potassium.
My friend, a Wolff White Parkinson ablatee has to eat keto to prevent rapid, debilitating PAC's from happening in high end exercise. Her story is written up here <[www.afibbers.org]
I’m a great fan of living this way. I can fast for days if I want. I always exercise fasted. I never have to stop to eat. My insulin levels are low as is my A1C. Is it for all afibbers – you have to evaluate your situation carefully and do your research.
George
For those who aren’t familiar. Here is a description of keto diets. This is by a type 1 diabetic, who is an MD and uses a keto diet to manage his diabetes: <[ketogenicdiabeticathlete.wordpress.com]
It has to do with electrolyte shifts that occur when someone transitions into a ketogenic state. This is a low insulin state. When insulin is high, the insulin signals the kidneys to conserve or retain sodium. When insulin drops to very low (and in my opinion, normal) levels, the kidneys are signaled to excrete sodium (called natriuresis of fasting). This can be dramatic enough that the body excretes potassium along with the sodium – trying to keep them in balance (body will secrete the hormone aldosterone causing it to excrete potassium). For more detailed explanation, see the books by Phinney and Volek <[www.artandscienceoflowcarb.com] They recommend supplementing with 5g/day of sodium, at lest 1g/day of potassium and also magnesium.
Most peoples’ ketone system are in “mothballs” since many fuel on a mostly carb diet to continually fill up the small glucose tank in the body. It can take up to 2 or more weeks of starvation or a very low carb (generally 20 or 30 g/day or less) diet with modest protein to stimulate the body to bring this system out of mothballs. The body first empties the glycogen stores in the muscles to feed the brain (which can only fuel on glucose or ketones). Once these are depleted, muscle protein is converted to glucose for this purpose (muscle tissue can fuel on fat). After a while the body starts making ketones from fat and these ketones can offset much of the brain’s need for glucose.
Ketones are not produced in a high insulin state.
In my case, I did not know about the sodium supplementation recommendation. I dropped my carb intake to around 20g/day. I got all the symptoms of “keto flu” (which can be mitigated with appropriate supplementation). After a few days, I noticed a “pounding heart” when I went to bed. This is typically a symptom of low potassium, so I loaded up on it – I don’t recall, but likely 4-5 grams/day. This continued for a couple of days. One evening I thought, this will lead to afib. Sure enough I woke up with 3 AM afib. I converted it in about an hour with 300 mg of flecainide (as usual). Except this time I converted to a rate of around 130 BPM (my normal rate after a flec conversion is in the 80’s). This stayed this way for a while. I got the idea to take a bunch of magnesium (as this was 6 years ago, don’t recall how much, likely 400-800 mg). I did and within 10 minutes, my rate started dropping into the 80’s. I took a while, but I think less than 30 minutes.
That was in Oct of 2009. I’ve been keto-adapted since, though have gone in and out of ketosis many times. I’ve yet to have another afib episode related to this. I also likely get less than 5 g/sodium/day. All food is cooked from scratch. I do add salt, but not a huge quantity.
As to why I think a low insulin diet is healthy. It starts with Dr. Joseph Kraft. You can read his book - <[www.amazon.com] A summary is here: <[www.thefatemperor.com] Bottom line – Kraft did 14,000+ oral glucose tolerance tests WITH insulin assays. He found that 80% who had normal glucose responses had abnormal insulin responses. He called this “diabetes in-situ.” This does not count all those who had abnormal glucose responses. You need a fasting insulin of 5 or less to be in the clear. Kraft also did 3,000 autopsies and saw that excess insulin was the cause of much calcification in the heart, its structures and blood vessels. So keeping insulin low is a hot option. Here is an interview with him – he’s 96 and first published on this around 1976. <[www.youtube.com] Catherine Crofts, in NZ, used the Kraft data for her PhD thesis recently. Here is a presentation by her : <[www.thefatemperor.com]
In this post, they cite a study demonstrating that fasting insulin represents 50% of total insulin secretion for the day. This relationship holds for those with low and high levels. Hence someone with a fasting insulin of 30 produces 10 times the insulin over the course of a day as someone with a fasting insulin of 3. <[www.buttermakesyourpantsfalloff.com]
The guys at Newcastle showed they could normalize glucose function by reducing fat around the pancrease (it is organ fat, not subcutaneous fat that is the issue) <[www.sciencedaily.com]
In Hans’ newsletter, the editor did n=1 experiments with the Newcastle approach. Here is a search on the archives: <[www.google.com]
Toronto doc, Jason Fung, talks about insulin and obesity <[intensivedietarymanagement.com]
And has a many part section on fasting, staring here: <[intensivedietarymanagement.com]
This is an old post, analyzing an older paper. <[high-fat-nutrition.blogspot.ie] However, he plotted the data to highlight the risk of coronary heart disease risk vs A1C levels
In summary – I think low insulin levels are a healthy way to live. As to afib, there is risk to going into ketosis. If you want to try it, make sure you pay attention to the electrolyte supplementation best practices. Can you get into ketosis slowly and mitigate the risk? I don’t know, I’ve not tried it. I have a friend who said she did. I’ve also read that it isn’t possible. I don’t know the answer. Will it help your afib? Perhaps, especially if you have comorbidities like hypertension and coronary artery disease. It was not a ticket out of afib for me. I already had that ticket to afib remission- primarily magnesium to bowel tolerance, but also taurine and earlier potassium.
My friend, a Wolff White Parkinson ablatee has to eat keto to prevent rapid, debilitating PAC's from happening in high end exercise. Her story is written up here <[www.afibbers.org]
I’m a great fan of living this way. I can fast for days if I want. I always exercise fasted. I never have to stop to eat. My insulin levels are low as is my A1C. Is it for all afibbers – you have to evaluate your situation carefully and do your research.
George
|
Re: Keto diets and afib April 27, 2016 01:18AM |
Registered: 8 years ago Posts: 1 |
I'd like to thank George for his thoughts and participation on this board. I would also like to thank Jackie as well as I have followed along for many years and , of course Hans. In short, I have had paroxymal A-fib since I have been 32. I'm now 55. My father has been on Rythmol for the past 35 years successfully. My brother was cardioverted twice in the last 4 months. I have been cardioverted 7 times in the last 23 years. I would considered myself a veteran in this struggle. I have resisted drug therapy as I am athletic and have been measured by holter as having a resting pulse during sleep of 29. My EP, who I went to elementary school with, thought any further reduction in my heart rate would not work well through drug therapy. So here I am 23 years later. No ablation. No drugs. I still push myself extensively through riding my mountain bike and going to the gym 350 days/year. I know,not popular on this forum. But , to be honest, none of you will challenge yourself in this way. It is much easier to assume it would be better to err on the side of safety and reduce exercise essentially that you have never entertained.
I digress, I started the Keto Diet 8 months ago. Theory being, a stable blood sugar level may help in my A-fib struggle. Just got my bloodwork back and my Triglerciride/HDL ratio is .15. where under 2.0 is considered good.This is now the standard for predicting heart disease. Do I have an answers? Hell no! But my heart has been quiet now for the last 6 months on Keto under my , which many would consider, severe exercise regimen.
My theory is A-fib is a symptom of several underlying problems. Not all of which originate from one source. Good luck in your search.
Cheers, J
I digress, I started the Keto Diet 8 months ago. Theory being, a stable blood sugar level may help in my A-fib struggle. Just got my bloodwork back and my Triglerciride/HDL ratio is .15. where under 2.0 is considered good.This is now the standard for predicting heart disease. Do I have an answers? Hell no! But my heart has been quiet now for the last 6 months on Keto under my , which many would consider, severe exercise regimen.
My theory is A-fib is a symptom of several underlying problems. Not all of which originate from one source. Good luck in your search.
Cheers, J
|
Re: Keto diets and afib April 27, 2016 03:17PM |
Registered: 7 years ago Posts: 18,886 |
Thank you, J, for the update. I appreciate learning of your great news.
It's long been known the Keto diet can be highly beneficial for many people and not just for reversing arrhythmia. You've certainly proven your discipline has paid huge dividends... not the least of which is avoiding an ablation... just as George (and others) have been able to do.
I totally agree that Afib is a symptom of an underlying problem although, unfortunately, it can be difficult to pinpoint and reverse it. I've long felt there is a gene mutation that contributes, as you note in your familial history, and you're doing just what is advised by the experts today using Epigenomics to overcome epigenomic mutations. The book by researcher, Jeffrey S. Bland, PhD, The Disease Delusion, offers welcome and substantial insight to using a ' functional systems management' approach to health problems.
Keep up the good work and do keep us posted periodically. Your story offers incentive to others.
Best to you,
Jackie
“The Disease Delusion provides critical insight into how environmental exposures to physical, chemical, and behavioral factors are linked to disease susceptibility through alterations in the epigenome, not simply in the genome. This revolutionary expansion in our understanding of the genesis of diseases promises to provide us with completely new approaches for preventing and treating human pathological conditions in the 21st century.”
—Randy Jirtle, PhD
Professor of Epigenetics at the Department of Sport and Exercise Sciences, University of Bedfordshire, Bedford, UK, and a Senior Scientist at McArdle Laboratory for Cancer Research, University of Wisconsin
[jeffreybland.com]
It's long been known the Keto diet can be highly beneficial for many people and not just for reversing arrhythmia. You've certainly proven your discipline has paid huge dividends... not the least of which is avoiding an ablation... just as George (and others) have been able to do.
I totally agree that Afib is a symptom of an underlying problem although, unfortunately, it can be difficult to pinpoint and reverse it. I've long felt there is a gene mutation that contributes, as you note in your familial history, and you're doing just what is advised by the experts today using Epigenomics to overcome epigenomic mutations. The book by researcher, Jeffrey S. Bland, PhD, The Disease Delusion, offers welcome and substantial insight to using a ' functional systems management' approach to health problems.
Keep up the good work and do keep us posted periodically. Your story offers incentive to others.
Best to you,
Jackie
“The Disease Delusion provides critical insight into how environmental exposures to physical, chemical, and behavioral factors are linked to disease susceptibility through alterations in the epigenome, not simply in the genome. This revolutionary expansion in our understanding of the genesis of diseases promises to provide us with completely new approaches for preventing and treating human pathological conditions in the 21st century.”
—Randy Jirtle, PhD
Professor of Epigenetics at the Department of Sport and Exercise Sciences, University of Bedfordshire, Bedford, UK, and a Senior Scientist at McArdle Laboratory for Cancer Research, University of Wisconsin
[jeffreybland.com]
|
Re: Keto diets and afib April 27, 2016 10:24PM |
Registered: 11 years ago Posts: 51 |
|
Re: Keto diets and afib May 01, 2016 02:32AM |
Registered: 9 years ago Posts: 171 |
|
Re: Keto diets and afib May 09, 2016 05:56AM |
Registered: 9 years ago Posts: 84 |
|
Re: Keto diets and afib February 20, 2017 12:02PM |
Registered: 7 years ago Posts: 1 |
Quote
OP
It can take up to 2 or more weeks of starvation or a very low carb (generally 20 or 30 g/day or less) diet with modest protein to stimulate the body to bring this system out of mothballs.
You can stimulate the whole ketogenic system by taking MCT oil for a period. MCT fats (C10, C8 and C6) will be broken up into ketone fuels (C2) even when diet is the normal mix of carbs, fat and protein.
Sorry, only registered users may post in this forum.